Lactation is one of the most remarkable physiological processes in women, providing essential nutrition and immunological protection to the newborn. The process of milk production, or lactogenesis, and its subsequent ejection, or milk let-down, are highly regulated by a complex interplay of endocrine and neuroendocrine factors. Understanding the hormonal regulation of lactation involves examining the key hormones involved, their sites of production, regulatory mechanisms, and how their actions can be pharmacologically manipulated to enhance milk production when necessary.
Anatomy and Physiology of the Mammary Glands
The mammary glands are specialized exocrine organs composed of lobes and lobules containing alveoli, which are the sites of milk synthesis. Each alveolus is lined with secretory epithelial cells, surrounded by contractile myoepithelial cells, and enveloped by a rich capillary network. Milk is synthesized in the epithelial cells and secreted into the alveolar lumen. The milk then travels through a ductal system, converging in lactiferous ducts that open at the nipple. Proper functioning of the mammary gland depends not only on the presence of secretory cells but also on vascular support, innervation, and the hormonal milieu that stimulates and sustains lactation.
The primary hormones involved in the regulation of lactation are prolactin and oxytocin, with additional modulatory roles played by estrogen, progesterone, insulin, cortisol, thyroid hormones, and growth hormone. Among these, prolactin and oxytocin are the central regulators, orchestrating milk synthesis and milk ejection, respectively.
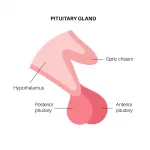
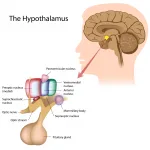
Prolactin, a peptide hormone, is the principal mediator of milk synthesis. It is synthesized and secreted by lactotroph cells in the anterior pituitary gland, located at the base of the brain within the sella turcica. The secretion of prolactin is predominantly regulated by hypothalamic factors, most notably dopamine, which acts as prolactin-inhibiting hormone. Dopamine is produced by neurons in the hypothalamic arcuate nucleus and tuberoinfundibular pathway and exerts a tonic inhibitory effect on prolactin secretion through D2 receptors on lactotrophs. This negative regulation is critical, as excessive prolactin secretion outside of pregnancy or lactation can lead to pathological conditions such as galactorrhea or hypogonadism.
During pregnancy, prolactin levels gradually rise due to estrogen-mediated proliferation of lactotrophs. Estrogen, secreted by the ovaries and the placenta, sensitizes the anterior pituitary to hypothalamic signals and primes the mammary glands for lactogenesis. Progesterone, also secreted by the placenta, plays an inhibitory role in milk secretion during gestation by suppressing the secretory activity of mammary alveolar cells despite high prolactin levels. This ensures that milk production does not commence prematurely. After delivery, the abrupt fall in progesterone and estrogen levels removes this inhibitory effect, allowing prolactin to stimulate milk synthesis effectively.
Prolactin acts directly on mammary alveolar epithelial cells by binding to prolactin receptors, which are members of the cytokine receptor superfamily. This binding activates the Janus kinase-signal transducer and activator of transcription (JAK-STAT) pathway, leading to transcriptional upregulation of genes encoding milk proteins, such as casein, lactalbumin, and lactoferrin. Additionally, prolactin promotes the synthesis of enzymes involved in lactose and lipid production, which are essential components of human milk. Importantly, prolactin secretion is not constant but follows a pulsatile pattern, with the highest levels occurring in response to suckling stimuli, which trigger a neuroendocrine reflex. Mechanoreceptors in the nipple transmit afferent signals via the spinal cord to the hypothalamus, leading to reduced dopaminergic inhibition and a consequent surge in prolactin release. This mechanism ensures that milk production is closely matched to the infant’s demand.
While prolactin stimulates milk production, it is oxytocin that mediates milk ejection or let-down. Oxytocin is synthesized in the hypothalamus, specifically in the paraventricular and supraoptic nuclei, and is transported to the posterior pituitary for storage and release. Oxytocin secretion is primarily triggered by the suckling stimulus and, to a lesser extent, by sensory stimuli such as the infant’s cry. Upon release into the systemic circulation, oxytocin binds to oxytocin receptors on the myoepithelial cells surrounding the alveoli and ductal system of the mammary gland. This binding induces contraction of the myoepithelial cells, forcing milk from the alveolar lumen into the ducts and toward the nipple. The milk ejection reflex is therefore a critical component of effective breastfeeding, as it allows the infant to receive milk efficiently and reinforces prolactin-mediated milk synthesis through continued nipple stimulation.
Several other hormones modulate the effects of prolactin and oxytocin on lactation. Thyroid hormones, including thyroxine (T4) and triiodothyronine (T3), are essential for normal metabolic support of the mammary gland and may enhance milk protein synthesis. Cortisol, secreted by the adrenal cortex, also plays a permissive role, supporting the differentiation and function of mammary epithelial cells. Insulin promotes the uptake of glucose and amino acids into mammary cells, providing substrates necessary for lactose and protein synthesis. Growth hormone contributes indirectly by modulating maternal metabolism and ensuring adequate nutrient supply for milk production. These modulatory hormones highlight the complex endocrine network that integrates systemic metabolic status with local mammary function.
Molecular Pathways in Lactation
The process of lactation is not merely a hormonal event but also a complex molecular orchestration at the cellular level. The effects of prolactin and oxytocin on milk synthesis and ejection are mediated by intracellular signaling cascades that regulate gene expression, protein synthesis, and cytoskeletal dynamics. Understanding these pathways provides insight into how endocrine signals are translated into functional outcomes in the mammary gland.
Prolactin Signaling Pathway
Prolactin exerts its effects primarily through the prolactin receptor (PRLR), a transmembrane receptor expressed on mammary epithelial cells. PRLR belongs to the class I cytokine receptor family and lacks intrinsic kinase activity. Upon prolactin binding, the receptor undergoes dimerization, which facilitates the recruitment and activation of Janus kinase 2 (JAK2), a cytoplasmic tyrosine kinase associated with the intracellular domain of PRLR. Activated JAK2 phosphorylates specific tyrosine residues on the receptor, creating docking sites for Signal Transducer and Activator of Transcription 5 (STAT5).
STAT5 is then phosphorylated by JAK2, dimerizes, and translocates to the nucleus, where it binds to specific promoter regions of milk protein genes, including β-casein, α-lactalbumin, and lactoferrin. This transcriptional activation increases mRNA levels for these proteins, which are subsequently translated in the endoplasmic reticulum and secreted into milk. STAT5 also regulates genes involved in lipid metabolism and lactose synthesis, ensuring coordinated production of all major milk components.
Beyond the JAK-STAT pathway, prolactin signaling activates other cascades, including PI3K/Akt and MAPK/ERK pathways, which modulate cell survival, proliferation, and differentiation of mammary alveolar cells. The PI3K/Akt pathway enhances glucose uptake and lipid synthesis, providing essential substrates for milk production, while MAPK/ERK contributes to cell proliferation and maintenance of the alveolar architecture during lactation.
Oxytocin Signaling Pathway
Oxytocin mediates milk ejection through its receptor, the oxytocin receptor (OXTR), a G-protein coupled receptor (GPCR) expressed on myoepithelial cells surrounding the alveoli. Binding of oxytocin to OXTR activates Gq/11 proteins, which stimulate phospholipase C (PLC). PLC hydrolyzes phosphatidylinositol 4,5-bisphosphate (PIP2) into inositol 1,4,5-trisphosphate (IP3) and diacylglycerol (DAG).
IP3 binds to its receptors on the endoplasmic reticulum, triggering the release of intracellular calcium stores. The rise in intracellular calcium concentration induces contraction of the actin-myosin cytoskeletal network in myoepithelial cells, resulting in the ejection of milk into the ductal system. DAG activates protein kinase C (PKC), which may further modulate cytoskeletal dynamics and enhance contractility. This precise molecular cascade ensures a rapid and coordinated milk let-down in response to the suckling stimulus.
Modulatory Hormone Pathways
Other hormones that modulate lactation also operate through defined molecular mechanisms. Estrogen binds to estrogen receptors (ERα and ERβ) in mammary epithelial and stromal cells, activating transcription of genes involved in mammary ductal growth and prolactin receptor expression. Progesterone, through the progesterone receptor (PR), antagonizes prolactin signaling by interfering with STAT5 transcriptional activity, which explains its inhibitory effect on milk synthesis during pregnancy. Insulin engages the insulin receptor (IR), a tyrosine kinase receptor, leading to activation of the PI3K/Akt pathway and facilitating nutrient uptake for lactose and lipid production. Cortisol acts via the glucocorticoid receptor (GR) to enhance transcription of milk protein genes, synergizing with prolactin to optimize milk synthesis.
Neuroendocrine Integration
Molecular signaling is also tightly integrated with neural inputs. Mechanosensitive afferent neurons in the nipple detect suckling and transmit signals to the hypothalamus, leading to dopamine inhibition and prolactin release. At the cellular level, this translates into increased JAK-STAT5 signaling in alveolar cells. Similarly, oxytocin neurons in the paraventricular and supraoptic nuclei respond to afferent input with bursts of oxytocin release, rapidly triggering calcium-dependent myoepithelial contraction.
Collectively, these molecular pathways illustrate how hormonal signals are transduced into precise cellular actions, coordinating milk synthesis and ejection. Dysregulation at any step—whether at the receptor level, signaling intermediates, or transcriptional control—can result in insufficient lactation, highlighting the importance of these pathways for both physiological and clinical understanding of breastfeeding.
Pharmacological interventions can be used to enhance milk production in women experiencing lactation insufficiency, a condition referred to as hypogalactia. Drugs that increase milk production are termed galactagogues, and they primarily target the prolactin pathway. One of the most commonly used galactagogues is domperidone, a dopamine D2 receptor antagonist. By blocking dopamine receptors on lactotrophs, domperidone removes the inhibitory effect of dopamine, thereby increasing prolactin secretion. Studies have demonstrated that domperidone can significantly elevate serum prolactin levels and enhance milk output in lactating women, particularly those with delayed lactogenesis or preterm infants. Another dopamine antagonist, metoclopramide, also increases prolactin levels and has been used as a galactagogue, though its central nervous system penetration can lead to side effects such as fatigue, depression, and extrapyramidal symptoms, making domperidone generally preferable.
Other pharmacological approaches target the oxytocin pathway, though these are less common. Synthetic oxytocin can be administered intranasally or intravenously to facilitate milk let-down in mothers with deficient oxytocin release, although its effect on actual milk synthesis is limited, as oxytocin primarily influences ejection rather than production. Additionally, some herbal or nutraceutical interventions, such as fenugreek or galactagogue teas, are purported to increase milk supply, though their efficacy is less well-established and likely involves indirect modulation of prolactin levels or maternal fluid intake.
It is important to note that pharmacological enhancement of lactation should be considered adjunctive to non-pharmacological measures, such as frequent and effective breastfeeding or pumping, ensuring adequate maternal nutrition, and addressing underlying medical or psychological conditions that may impair lactation. The interplay between endocrine signaling, maternal-infant interaction, and environmental factors underscores the multifaceted nature of lactation regulation.
In summary, the regulation of milk production in women is orchestrated by a finely tuned hormonal network centered on prolactin and oxytocin. Prolactin, produced by anterior pituitary lactotrophs and inhibited by hypothalamic dopamine, drives milk synthesis in the alveolar epithelial cells through activation of the JAK-STAT pathway and upregulation of milk protein and lactose-producing enzymes. Oxytocin, synthesized in the hypothalamus and released from the posterior pituitary, mediates milk ejection via contraction of myoepithelial cells. Additional hormones, including estrogen, progesterone, thyroid hormones, insulin, cortisol, and growth hormone, provide necessary modulation, ensuring that milk production is responsive to maternal physiology and infant demand. Pharmacological strategies to enhance lactation, primarily through dopamine antagonists such as domperidone, can effectively increase prolactin levels and milk output, providing critical support for mothers experiencing lactation insufficiency. The integration of hormonal control, neuroendocrine reflexes, and clinical interventions illustrates the sophisticated biological orchestration underlying successful human lactation.
Overall, understanding the hormonal regulation of lactation provides a foundation for both basic physiological knowledge and clinical applications. It emphasizes the importance of prolactin and oxytocin as central regulators, the role of modulatory hormones in fine-tuning lactation, and the potential for pharmacological intervention when natural processes are insufficient. Effective lactation not only sustains neonatal growth and immunity but also reflects the remarkable adaptability of the maternal endocrine system, demonstrating a finely balanced network of hormonal, neural, and environmental factors working in concert to support one of the most fundamental aspects of human reproduction.

Leave a Reply